The conference was held by BI company at Le Méridien Taichung. The medication used in the case sharing were mostly from BI company. The speakers and moderators were all expertise in diabetes and kidney disease.
Dr. Tu from Ray Tong Clinic shared 5 cases with diabetes and kidney disease. To protect the privacy of the patients, only important thinking process and treatment courses are shared in the page.

This is a case of chronic kidney disease for years.
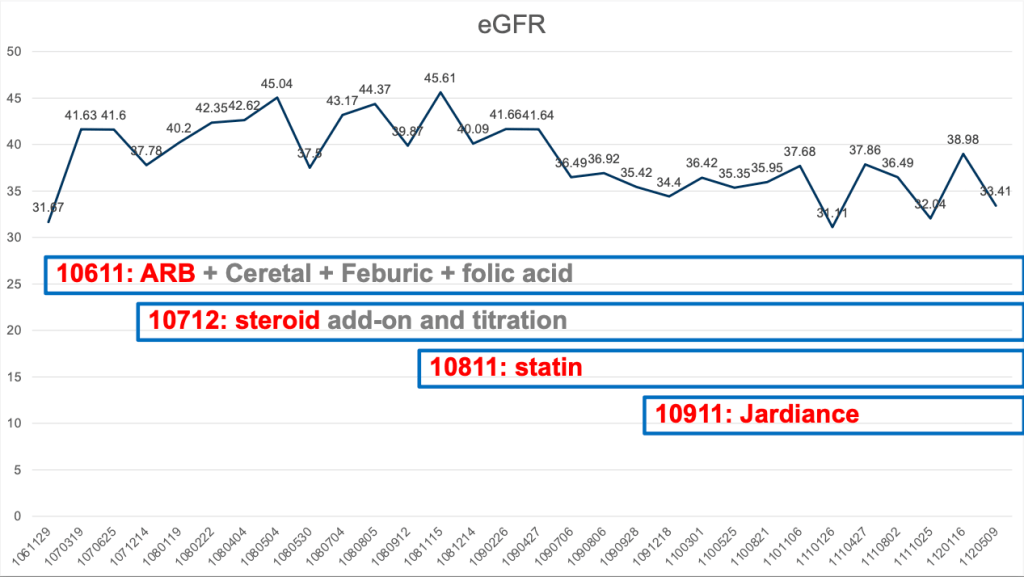
As you can see from the graph below, he has been under regular follow-up in our clinic for near 6 years with relative stable eGFR level.
He was initially under ARB, ceretal, for proteinuria, feburic acid for hyperuricemia and gout, folic acid for CKD and prevention of CVA.
Since 201812, steroid was initiated and under careful titration according to the urine protein level.
One the other hand, statin was also prescribed since 201911 to prevent CV events.
Last but not the least, SGLT2 i was initiated since 202011 after more and more solid evidence from SGLT2i in view of prevention and treatment for CKD and heart failure in patients with T2D, CKD and heart failure.
Fluctuation of HbA1c level was noted during the course of treatment, especially after the start of steroid use.

Dramatic drop of urine ACR was noted under the treatment of ARB, ceretal, Steroid, and Jardiance.
The more the proteinuria, the more risk of CKD progression will be.
Proteinuria is the most important treatment target in the care of CKD patients.
RAAS blockades and SGLT2 i are the two most important agents to treat and prevent CKD progression, followed by non-steroidal MRA, which emerges as one of the choices for DKD patients with residual proteinuria.

